|
On November 1, 2022, the Centers for Medicare & Medicaid Services (CMS) released the calendar year (CY) 2023 Medicare Physician Payment Schedule (MPS) and Quality Payment Program (QPP) final rule that impacts payments for physicians and other health care practitioners. CMS had issued a proposed rule in July, which the AMA responded to with a robust set of comments. There are a number of policies in the 2023 MPS and QPP final rule that the AMA strongly supports. Below are some of the highlights from our initial read of the final rule, indicating our support, opposition, or need for improvement. CALENDAR YEAR 2023 UPDATES TO THE MEDICARE PHYSICIAN PAYMENT SCHEDULE Conversion Factor and Medicare Economic Index (MEI) The finalized CY 2023 Medicare conversion factor is $33.06, a decrease of $1.55 or 4.5% from the 2022 CF of $34.61. The decrease is largely a result of an expiring 3% increase funded by Congress through 2022. The additional approximate 1.6% decrease is the result of budget neutrality requirements that stem from the revised E/M changes. The AMA and the Federation are strongly advocating that Congress avert this payment cut, as well as implement an inflationary update for physicians, extend the five percent Advanced APM incentive and prevent the steep increase to the participation requirements for APMs, and waive the four percent PAYGO sequester. Rebasing and Revising the MEI CMS has finalized the Medicare Economic Index (MEI) weights for the different cost components of the MEI. The current MEI weights are based primarily on results from the AMA’s PPI survey, based on 2006 data. CMS used data from the Census Bureau’s Service Annual Survey (SAS) as the primary source for the new weights. CMS supplemented the SAS data with other sources when SAS does not provide the necessary detail. The changes lead to substantial changes in the weights for many of the key components of physician practice expense. For example, the weight for non-physician compensation increases from 16.6% in the current MEI to 24.7% in the new MEI, and the weight for professional liability insurance decreases from 4.3% to 1.4 %. CMS will not implement the MEI changes in 2023, referencing the need for continued public comment due to the significant impact to physician payments. CMS also states that they will be interested to compare the results of the AMA practice expense data collection effort to the data used in their new MEI calculation. The MEI is used to proportion the components of the RBRVS between work, practice expense, and professional liability insurance (PLI). The current and proposed proportions of payment would be as follows based on the updated MEI: 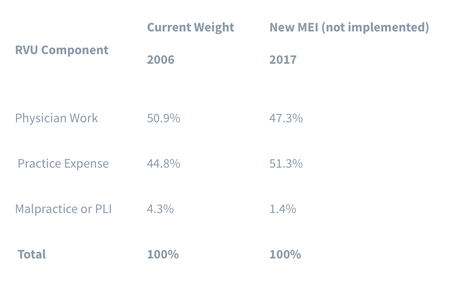 Telehealth
CMS finalized its proposal to extend telehealth coverage for an additional five months beyond the end of the PHE for the codes that were only going to be on the telehealth list through the end of the PHE. CMS agreed to maintain the same payment rates for office visits provided in-person or via telehealth through the end of 2023 instead of reducing payments for telehealth visits to the facility rates. Evaluation and Management (E/M) Visits CMS adopted the revised CPT guidelines and codes and the AMA/Specialty Society RVS Update Committee (RUC) recommended relative values for additional E/M visit code families, including hospital visits, emergency department visits, home visits and nursing facility visits. These changes allow time or medical decision-making to be used to select the E/M visit level. CMS also finalized creation of Medicare-specific coding for payment of Other E/M prolonged services, similar to what CMS adopted in CY 2021 for payment of Office/Outpatient prolonged services. These services will be reported with three separate Medicare-specific G codes. Split or Shared Visits In response to advocacy from the AMA and 46 national medical specialty societies, CMS finalized a one-year delay of its policy requiring a physician to see the patient for more than half of the total time of a split or shared E/M visit in order to bill for the service. CMS will continue to allow physicians and qualified health care professionals to use history, physical exam, medical decision making (MDM), or more than half of the total time spent with a patient to determine the substantive portion of the split/shared visit in 2023. Chronic Pain Management and Treatment Services CMS finalized new HCPCS codes, G3002 and G3003, and valuation for chronic pain management and treatment services (CPM) for CY 2023 and provided some additional flexibilities, such as the ability to report CPM and other visits on the same date and to report subsequent CPM services as many times as needed in a month. Final rule excerpt on CPM Services G-codes
To appropriately price methadone for CY 2023 and subsequent years, CMS is finalizing the proposal to revise its methodology for pricing the drug component of the methadone weekly bundle and the add-on code for take-home supplies of methadone, which will increase the 2023 rate by 5.3%. CMS is also finalizing the proposal to allow the OTP intake add-on code to be furnished via two-way audio-video communications technology when billed for the initiation of treatment with buprenorphine, to the extent that its use of audio-video to initiate treatment with buprenorphine is authorized by the Drug Enforcement Administration (DEA) and Substance Abuse and Mental Health Services Administration (SAMHSA) at the time the service is furnished. CMS will also allow audio-only technology to be utilized for intake in cases where audio-video is not available to the patient, and CMS will allow audio-only technology for periodic assessments through 2023. QUALITY PAYMENT PROGRAM (QPP) AND MERIT-BASED INCENTIVE PAYMENT SYSTEM Merit-based Incentive Payment System (MIPS) Value Pathways CMS finalized five new and seven revised MIPS Value Pathways (MVPs), a new participation option beginning in 2023. The 12 voluntary MVP options for 2023 are:
Subgroup Reporting Subgroup reporting will be an option for MVP participants beginning in 2023. Despite concerns raised by the AMA and other stakeholders, CMS finalized its proposal to require multispecialty groups that choose to report through an MVP to participate as subgroups beginning in 2026. CMS finalized its proposal to limit an individual physician to one subgroup. The agency will score subgroups on population health administrative claims measures and cost measures based on their affiliated group score and, if there is no group score, the administrative claims measures and cost measures would be excluded from the final score. Finally, CMS will not assign a score for subgroups that register but do not submit data for an applicable performance period. Merit-based Incentive Payment System (MIPS) Performance Threshold Despite the AMA raising alarms due to CMS’ estimate that one-third of MIPS-eligible clinicians would receive a penalty, CMS finalized its proposal to maintain the MIPS performance threshold, which is the minimum score necessary to avoid a penalty, at 75 points. Under MACRA, the $500 million exception performance bonus expires in payment year 2024, so 2023 will be the first performance period without a corresponding exceptional performance bonus and exceptional performance threshold. In other words, the only bonuses available for 2023 MIPS participants will be budget neutral bonuses resulting from penalties to physicians and groups that score fewer than 75 points. Projected 2023 MIPS Participation and 2025 Payment Adjustments CMS estimates that 719,516 physicians and qualified health care professionals will be MIPS eligible in the 2023 performance period. The agency projects that about two-thirds of MIPS eligible clinicians who submit some data to CMS would receive a positive or neutral payment adjustment in 2025 based on the 2023 performance period. Many scores are expected to be close to the performance threshold of 75 points, so the number of eligible clinicians who receive bonuses and penalties may differ from these estimates. Among engaged clinicians, which are those who submit any MIPS data, the average positive payment adjustment is estimated to be 3.71 and the average penalty is estimated to be -1.81. The maximum bonus would be 6.09 percent, and the maximum penalty would be -9 percent. CMS projects that 8.5 percent of eligible clinicians would receive a score of less than 50 points, resulting in a penalty of more than -3 percent. Qualifying Alternative Payment Model Participants (QP) Under statute, the 5% incentive payment for QPs expires at the end of the 2022 performance period. In addition, the thresholds to achieve QP status beginning in the 2023 performance period will increase to 75% for the payment amount, and 50 percent for patient count. Based on these statutory changes, CMS estimates that between 144,700 and 186,000 eligible clinicians would become QPs in the 2023 performance period, and therefore be excluded from MIPS. This is a reduction from the 271,276 eligible clinicians who earned QP status in 2021. The AMA is strongly urging Congress to extend the 5% APM incentive payment and to continue to allow the Secretary flexibility to set the QP thresholds, including joining the National Association of ACOs and others stakeholders to form the new Alliance for Value-Based Care to amplify the necessity to continue these policies to support physicians and other providers who are redesigning care and taking on financial risk to improve patient outcomes and curb cost growth.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
AuthorWrite something about yourself. No need to be fancy, just an overview. Archives
June 2024
Categories |
 RSS Feed
RSS Feed